




























Step 5 of 16
Atrioventricular canal (AV canal) defects
An AV canal defect (endocardial cushion defect) is an absence of septation in the centre of the heart. It consists of an ostium primum-type ASD, an inlet VSD, and a 5-leaflet atrioventricular valve surrounding a central orifice (Videos and Figure 15.21). It exhibits five characteristics.
- Low ASD located on the septum (ostium primum);
- VSD located below the tricuspid valve (inlet VSD);
- Excessively apical insertion of the mitral annulus (mitral and tricuspid valves in the same plane);
- Cleft in the septal leaflet of the tricuspid valve and in the anterior leaflet of the mitral valve (Vidéo Canal AV) – these clefts cause regurgitation into the atrium;
- Gooseneck deformity of the LV outflow tract due to the apical position of the mitral annulus in relation to the aortic annulus.
Video: 4-chamber view of an AV canal, with typical insertion of tricuspid and mitral valves on the same plane at the level of the septum; presence of an ASD ostium primum.
Video: 4-chamber view of an AV canal, with typical insertion of tricuspid and mitral valves on the same plane at the level of the septum; presence of a VSD at the level of the admission chamber.
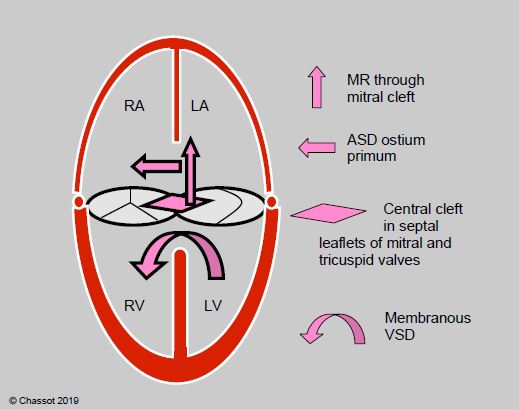
Figure 15.21: Diagram of the AV canal defect. There is an ostium primum-type ASD (horizontal arrow), a perimembranous VSD (curved arrow), a cleft in the septal leaflets of the tricuspid valve and the mitral valve (rhombus), and mitral leakage through the cleft in the anterior leaflet (vertical arrow). This results from non-fusion of the atrial septum, interventricular septum and two atrioventricular valvular cushions (endocardial cushion defect). MR: mitral regurgitation.
These different orifices communicate between each other, and shunting may occur in numerous directions: LV→RV, LV→RA, LA→RA, LA→RV. Clefts are associated with mitral insufficiency (LV→LA) and tricuspid insufficiency (RV→RA) (Figure 15.22) (Videos).
Video: 4-chamber view of an AV canal with colour flow, showing a double mitral regurgitation (through the commissure and through the cleft near the septum), and a tricuspid regurgitation.
Vidéo: Complex diastolic flow between LA, RA and RV in an AV canal.

Figure 15.22: Images of flows through an AV canal defect. A: two mitral regurgitations – one through the cleft (green arrow) and the other through the physiological commissure (yellow arrow, MI). B: two valve insufficiencies through different clefts – one through the septal leaflet of the tricuspid valve (TI) and the other through the anterior leaflet of the mitral valve (green arrow). They are separated by the atrial septum.
In some cases, the AV canal defect is partial and only includes one ASD with or without a cleft or a VSD without any atrial lesions. In echocardiography, the tricuspid and mitral valves are typically located in the same plane and inserted at the same level on the septum ( Figure 15.23; see Figure 15.2) [3].
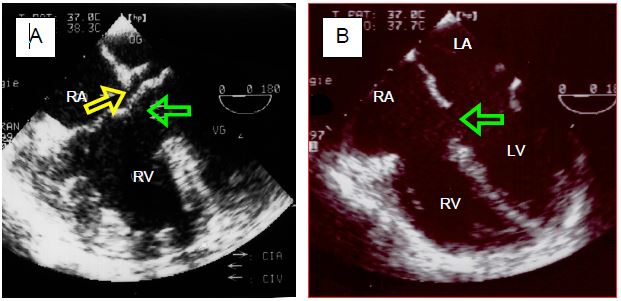
Figure 15.23: TEE image of the AV canal defect. A: combination of an ASD located very low between the atria (ostium primum-type) (yellow arrow) and a high VSD (inlet-type) (green arrow). The septal insertions of the tricuspid valve and mitral valve are in the same plane – the RV is highly hypertrophied due to pulmonary hypertension linked to the wide VSD. B: Ostium primum-type ASD (green arrow) – this is in fact a partial AV canal defect. The RV only exhibits dilation linked to volume overload due to the ASD.
An AV canal defect is associated with Down syndrome in 35% of cases [5]. Its clinical presentation is determined by the dominant lesion, which is a VSD in most cases. The RA is dilated, the RV and LV are hypertrophied and dilated. The risk of PAH is much higher than for ASDs due to the presence of a VSD. Pulmonary hypertension develops quite early in disease progression and is proportionate to the size of the VSD. Long-term complications of surgical correction performed in childhood are persistent mitral regurgitation, sub-aortic dynamic stenosis (obstruction of the left outflow tract) and AV block.
Surgical correction of AV canal defects is indicated to reduce the mitral regurgitation, close the shunt if the Qp/Qs is > 1.5, and widen the LVOT if the maximal gradient is > 50 mmHg [6]. It entails closing the ASD and VSD with patches and repairing leaflets presenting a cleft. Closure by percutaneous catheterisation is not possible [1]. The post-correction echocardiographic examination must focus on the competence of the mitral and tricuspid valves and a search for any residual leakage around the patches. Small residual leaks generally disappear spontaneously, especially after administration of protamine – only significant leaks justify reoperation. A comparison of saturation levels in the IVC and SVC with those of the PA gives an indication of the extent of any residual shunting caused by these leaks. The rate of reoperation in adults following a correction performed in childhood is very high (11-32%) [4]. Reoperation after AV canal defects is very common, representing 10% of cardiac surgery in adult congenital heart disease patients [2]. The most common causes of reoperation are mitral or tricuspid insufficiency, residual L-to-R shunting, obstruction of the LVOT (mean gradient > 50 mmHg) and LV dysfunction [2,7]. The long-term survival rate post-reoperation is 88% [4]. The correction of AV canal is contra-indicated if PVR are > 0.65 SVR, if sPAP is > 0.65 sAP, and if shunt is R-to-L [6].
Anaesthesia
Challenges facing anaesthetists relate chiefly to VSDs, pulmonary hypertension (see VSD and Pulmonary hypertension), and any stenosis of the left outflow tract or RV or LV dysfunction. In the event of an isolated ostium primum, haemodynamic behaviour is the same as for a simple ASD.
| Atrioventricular canal (AVC) defects |
| Lack of central septation of the heart associated with: - Ostium primum ASD - Inlet VSD - Complex shunting between LA-RA, LV-RV, LA-RV - Cleft in the septal leaflet of the tricuspid valve and in the anterior leaflet of the mitral valve with tricuspid and mitral insufficiencies - Gooseneck deformity of the LVOT If a major VSD is present: high risk of PAH and LV dysfunction. If the VSD is minimal, progression is the same as for an ASD or MI. The rate of reoperation in adults following a correction performed in childhood is high. |
© BETTEX D, CHASSOT PG, January 2008, last update February 2020
References
- BAUMGARTNER H, BONHOEFFER P, DE GROOT NMS, et al. ESC Guidelines for the management of grown-up congenital heart disease (new version 2010). Eur Heart J 2010; 31:2915-57
- BERGIN ML, WASHES CA, TAJIK AJ, et al. Partial atrioventricular canal defect: long term follow-up after initial repair in patients ≥ 40 years old. J Am Coll Cardiol 1995; 25:1189-94
- CHASSOT PG, BETTEX D. Perioperative transoesophageal echocardiography in adult congenital heart disease. In: POELAERT J, SKARVAN K. Transoesophageal echocardiography in anaesthesia. London, BMJ Book, 2004
- HOOHENKERK GJ, BRUGGEMANS EF, KOOLBERGEN DR, et al. Long-term results of reoperation for left atrio-ventricular valve regurgitation after correction of atrio-ventricular septal defects. Ann Thor Surg 2012; 93:849-55
- PICCOLI GP. Morphology and classification of complete atrioventricular defects. Brit Heart J 1979; 42:633-9
- STOUT KK, DANIELS CJ, VALENTE AM, et al. 2018 AHA/ACC Guideline for the management of adults with congenital heart disease. J Am Coll Cardiol 2019; 73:e81-192
- WARNES CA, WILLIAMS RG, BASHORE TM, et al. ACC/AHA 2008 Guidelines for the management of adults with congenital heart disease: executive summary. Circulation 2008; 118:2395-451
15. Anesthesia for adult congenital heart disease patients
- 15.1 Introduction
- 15.2 Nomenclature and pathophysiology
- 15.3 Approach by pathology
- 15.3.1 Classification
- 15.3.2 Diagnostic methods
- 15.3.3 Anomalous venous returns
- 15.3.4 Atrial septal defects (ASDs)
- 15.3.5 Atrioventricular canal (AVC) defects
- 15.3.6 Ebstein anomaly
- 15.3.7 Ventricular septal defects (VSDs)
- 15.3.8 Ventricular hypoplasia
- 15.3.9 Tetralogy of Fallot
- 15.3.10 Mixed shunt
- 15.3.11 Pulmonary stenosis
- 15.3.12 Anomalies of the LV ejection pathway
- 15.3.13 Transposition of the great arteries (TGA
- 15.3.15 Coarctation of the aorta
- 15.3.14 Congenitally corrected TGA
- 15.3.16 Arterial abnormalities
- 15.4 General considerations for anesthesia
- 15.5 Conclusions