




























Step 7 of 9
Impact of TEE
There are four areas in which TEE can be of use in the operating theatre and intensive care [2,6]:
- Assessing congenital heart disease patients’ complex anatomy and haemodynamics;
- Assessing ventricular function and blood volume;
- In cardiac surgery, a pre-correction examination reveals unexpected lesions in 7% of cases;
- A post-correction examination (post-CPB) justifies immediate reoperation for residual lesions in 8% of cases.
TEE is used both in the catheterisation room and operating theatre or intensive care. In addition to a transthoracic exam, it helps define posterior lesions (anomalous venous return), septal lesions (ASD, VSD, AV canal defects) or mitral lesions. It is essential for guiding endovascular procedures (valve dilation, ASD occlusion) and complex reconstructions. Besides the additional data it provides, TEE is very useful to anaesthetists and intensive care specialists for understanding these pathologies’ haemodynamics and assessing ventricular function, blood volume and myocardial ischaemia [7]. This is particularly important since the customary functional indicators and filling pressures are ineffective in these situations. After correction with CPB, it can be used to immediately check whether surgery has been successful.
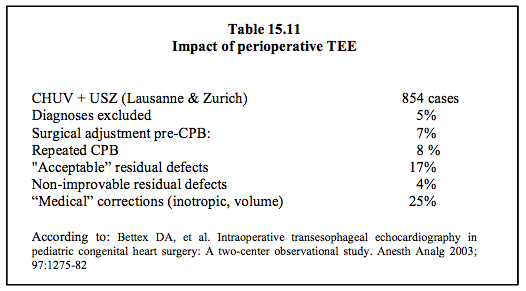
The clinical impact of TEE varies depending on the pathology. It is particularly useful in cases of obstructed right or left ventricular outflow tract, valve repair or atrioventricular discordance [8]. It enables immediate diagnosis of residual leakage after correction of shunts or stenosis, and after performing anastomoses or conduits. In cases of coronary reimplantation, TEE is necessary for assessing ventricular segmental wall function and diagnosis of myocardial ischaemia. In such cases, it is easy to complete the correction or repair the residual lesion during the same operating period, thus avoiding a second operation (Table 15.11). The fact that this occurs in 8-14% of cases means that perioperative TEE is medically indispensable and cost-effective [5].
The clinical impact of TEE varies depending on the pathology. It is particularly useful in cases of obstructed right or left ventricular outflow tract, valve repair or atrioventricular discordance [8]. It enables immediate diagnosis of residual leakage after correction of shunts or stenosis, and after performing anastomoses or conduits. In cases of coronary reimplantation, TEE is necessary for assessing ventricular segmental wall function and diagnosis of myocardial ischaemia. In such cases, it is easy to complete the correction or repair the residual lesion during the same operating period, thus avoiding a second operation (Table 15.11). The fact that this occurs in 8-14% of cases means that perioperative TEE is medically indispensable and cost-effective [5].
TEE is useful under all circumstances for assessing and correcting patients’ blood volume and individual ventricular function [5]. This is particularly true of congenital patients since their haemodynamics are very unusual: with their peculiar anatomy, pressure measurements do not genuinely reflect ventricular filling or systolic function. Moreover, the geometric approximations used to calculate ejection fraction are inappropriate for these remodelled ventricles, whose loading conditions are very unusual [3]. It is prudent to perform volume measurements of the chambers in two perpendicular planes in order to calculate LV ejection fraction (Simpson's rule) or use new 3D technologies to assess the RV.
The impact of TEE on congenital cardiac surgery has mainly been analysed in paediatrics. However, everything indicates that it is just as important for adult congenital surgery. The incidence of fortuitous findings and changes to surgical strategy is higher in congenital heart patients than among patients with acquired lesions. Prior to CPB, it fluctuates between 3% and 13% (mean: 7%) [5,7,8]. A second run of CPB based on an unsatisfactory TEE image occurs in 5 to 16% of cases (mean: 8%). This incidence is highest in complex pathologies, valve repairs and outflow tract lesions.
Some comments should be made with regard to the decision to perform a second run of CPB following a correction that is deemed unsatisfactory.
- Undiagnosed residual lesions are one of the main causes of postoperative complications, subsequent reoperation, and poor long-term survival.
- In 4% of cases, residual lesions cannot be corrected without causing major damage. They must be tolerated despite their consequences.
- Due to its high sensitivity, TEE reveals many lesions that have no clinical significance (mean: 15% of cases) [5,9,11]. A large experience is often required to distinguish between those that entail long-term consequences and those that are unimportant.
- The aim of surgery is to achieve an adequate surgical outcome and not a perfect echocardiographic image (Treat the patient, not the image!). Performing a second run of CPB to correct an inconsequential defect shows poor judgement of risk.
- The significance attributed to post-CPB findings is directly related to the examiner’s echocardiographic knowledge – the reoperation rate for incomplete correction falls from 9.6% to 0% and the incidence of undiagnosed lesions increases from 21% to 74% if a senior echocardiographer is replaced by a colleague with no experience [10].
The cost-effectiveness of routine TEE is very favourable among congenital heart disease patients. This has been calculated in paediatric heart surgery. Based on 5% incidence of immediate reoperation post-CPB and on the complexity of the various cases, financial analysis of TEE use shows that TEE enables savings of €700 to €2,200 per case, which covers any necessary investment [1,4].
© BETTEX D, CHASSOT PG, January 2008, last update May 2018
References
| Impact of TEE |
| There are four areas in which TEE can be of use in the operating theatre and intensive care: - Assessing congenital heart disease patients’ complex anatomy and haemodynamics - Assessing ventricular function and blood volume - Examination prior to correction (pre-CPB): unexpected lesions in 7% of cases - Examination after correction (post-CPB): immediate reoperation justified in 8% of cases Fortuitously detected lesions have no therapeutic significance in 15% of cases. The effectiveness of TEE in congenital heart disease patients is directly linked to the examiner’s knowledge. |
© BETTEX D, CHASSOT PG, January 2008, last update May 2018
References
- BENSON MJ, CAHALAN MK. Cost-benefit analysis of transesophageal echocardiography in cardiac surgery. Echocardiography 1995; 12:171-83
- BETTEX D, CHASSOT PG. Transesophageal echocardiography in congenital heart disease. In: BISSONNETTE B, edit. Pediatric anesthesia. Basic principles, State of the art, Future. Shelton (CO): People’s Medical Publishing House (USA), 1186-1212
- BETTEX DA, HINSELMANN V, HELLERMANN JP, JENNI R, SCHMID ER. Inaccuracy of cardiac output determination by transoesophageal echocardiography. Anaesthesia 2004; 59:1184-92
- BETTEX DA, PRETRE R, JENNI R, SCHMID ER. Cost effectiveness of routine intraoperative transesophageal echocardiography in pediatric cardiac surgery: a ten-year experience. Anesth Analg 2005; 100:1271-5
- BETTEX DA, SCHMIDLIN D, BERNATH MA, PRETRE R, HURNI M, CHASSOT PG. Intraoperative trasnesophageal echocardiography in pediatric congenital heart surgery: A two-center observational study. Anesth Analg 2003; 97:1275-82
- CHASSOT PG, BETTEX D. Perioperative transoesophageal echocardiography in adult congenital heart disease. In: POELAERT J, SKARVAN K. Transoesophageal echocardiography in anaesthesia. London, BMJ Book, 2004
- MILLER-HANCE WC, SILVERMAN NH. Transesophageal echocardiography (TEE) in congenital heart disease with focus on the adult. Cardiol Clinics 2000; 18:861-92
- RANDOLPH GR, HAGLER DJ, CONNOLLY HM, et al. Intraoperative transesophageal echocardiography during surgery for congenital heart defects. J Thorac Cardiovasc Surg 2002; 124:1176-82
- ROSENFELD HM, GENTLES TL, WERNKOVSKY G, et al. Utility of intraoperative echocardiography in the assessment of residual cardiac defects. Ped Cardiol 1998; 19:346-51
- STEVENSON JG. Adherence to physician training gudelines for pediatric transesophageal echocardiography affects the outcome of patients undergoing repair of congenital cardiac defects. J Am Soc Echocardiogr 1999; 12:165-72
- UNGERLEIDER RM, KISSLO JA, GREELEY WJ, et al. Intraoperative echocardiography during congenital heart operations: Experience from 1000 cases. Ann Thorac Surg 1995; 60:S539-42
15. Anesthesia for adult congenital heart disease patients
- 15.1 Introduction
- 15.2 Nomenclature and pathophysiology
- 15.3 Approach by pathology
- 15.3.1 Classification
- 15.3.2 Diagnostic methods
- 15.3.3 Anomalous venous returns
- 15.3.4 Atrial septal defects (ASDs)
- 15.3.5 Atrioventricular canal (AVC) defects
- 15.3.6 Ebstein anomaly
- 15.3.7 Ventricular septal defects (VSDs)
- 15.3.8 Ventricular hypoplasia
- 15.3.9 Tetralogy of Fallot
- 15.3.10 Mixed shunt
- 15.3.11 Pulmonary stenosis
- 15.3.12 Anomalies of the LV ejection pathway
- 15.3.13 Transposition of the great arteries (TGA
- 15.3.15 Coarctation of the aorta
- 15.3.14 Congenitally corrected TGA
- 15.3.16 Arterial abnormalities
- 15.4 General considerations for anesthesia
- 15.5 Conclusions